Some of us don’t do acronyms.
1 Like
Ah, yes, that makes sense. Now if we only knew break-through age distribution to reassure me 
And yes, CFR in this context is Case Fatality Rate.
Ahem 
1 Like
Because nobody cares if you get a mild case? And most people aren’t going to get tested without good reason?
There will be lots of people who never test positive because they never get tested. Why would they? They got vaccinated, they haven’t changed their behavior much, and if the symptoms are mild, why would they test?
I don’t think “mild case” data is going to be very useful.
4 Likes
This is a good point.
The vaccination rate is higher for higher ages:
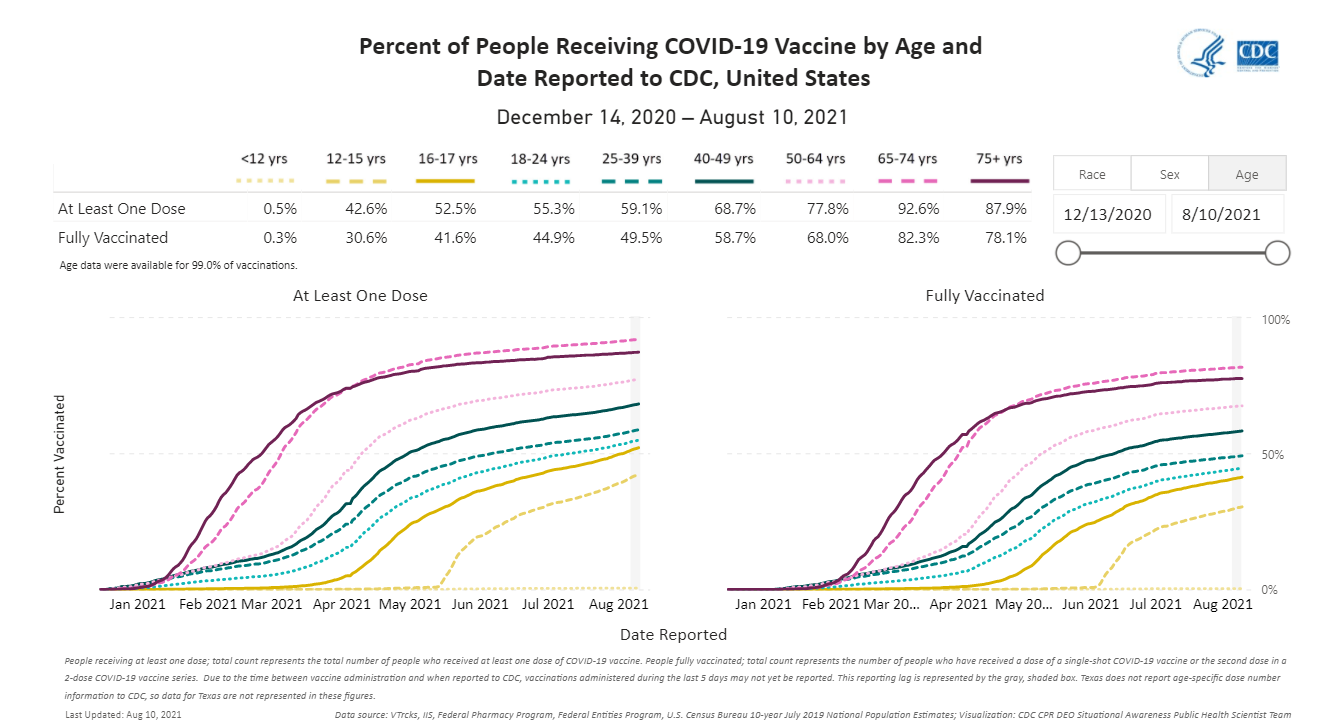
Though highest rate is for those age 65-74, which makes a little sense. Those folks are mostly mobile. The over age 75 group has a lot of people who go nowhere, unless somebody takes them. If nobody takes them to get vaccinated, they can’t take themselves. It’s still pretty high for that group, though.
Getting back to that base rate fallacy issue, the vaccinated population is going to skew higher than the unvaccinated population. The CFR in unvaccinated people in the earlier COVID strains showed the usual Gompertz-Makeham form:
So that means that even if vaccination reduced CFRs by 90%, it would likely be the young unvaccinated still have lower COVID CFRs than the old vaccinated people.
The usefulness to me is answering the question “Does the vaccine really reduce CFR for the elderly?”, which in turn allows me to advise my mom on how cautious she needs to be to avoid COVID, since it isn’t clear how much vax will reduce transmissibility (with Delta seemingly reducing vax effectiveness). If “mild-case” underreporting is similar for unvax/vaxxed cases, then I don’t have to know about “mild-case”.
But you are right, we won’t have a widespread monitoring system when threat isn’t significantly higher than it is now. People are just burnt out. Plus, it might not be cost effective depending on monitoring mechanism. Welcome to the “live with it” portion of our pandemic.
Plus there’s this (agreeing with you):
This seems relevant to your question:
And this one (same author):
1 Like
Google tried to tell me it was Code of Federal Regulations. That didn’t make much sense in context. Case Fatality Rate makes much more sense.
Here an article that says Moderna may be better than Pfizer/BioNTech and that it seems immunity wanes. https://www.cnbc.com/2021/08/09/moderna-may-be-superior-to-pfizer-against-delta-variant-breakthrough-odds-rise-with-time.html
Another one indicated that hospitalizations and deaths among breakthrough cases seem to be demographically the same as we have seen in all cases. The old and immunocompromised are most at risk.
We’re not at that point yet, although we should be. The CDC has continued to recommend asymptomatic testing for unvaccinated people (which explains the roughly 45% of pediatric covid “hospitalizations” that are really incidental infections) but have recommended (I’ve lost track of what their current recommendation is) not doing routine screening testing of the vaccinated.
The reason it won’t be useful will be because of all the people who never got tested. That was my main meaning. Yes, if we could show that vaccinated people “in the wild” who were exposed have much milder results, that would be great.
But I was thinking through what people actually do.
In my own family, the only people who have ever been tested for COVID are the 2 people who needed it in order to do certain things. The rest of us just tested ourselves for symptoms (mainly: loss of smell, which is easy to test (we’ve got some really pungent oils I have for aromatherapy and I can smell those even with a bad cold), but also fever and low oxygenation), and as we never had the key symptoms, we never got tested.
So, by its very definition, most mild cases will be missed unless there’s a reason people would get tested.
-sigh-
I assume with vaccination, you still get the same relative risks between groups (who are vaccinated). So all age groups, say, could see hospitalizations, deaths, etc., reduced 90% proportionately… and having the observation you mention.
It’s like the idiotic person who noticed that the distribution of deaths among ages were the same (more-or-less) as in normal years! Therefore, this is bullshit!
I pointed out that death rates could be doubled for each age group, and you’d get the same result. But a doubling of death rates wouldn’t be bullshit. [note: death rates didn’t double, but it was a large increase]
Likewise, it doesn’t really matter that you get the same distribution of ages/comorbidities among hospitalizations and deaths among vaccinated as non-vaccinated.
For those who missed it:

I’m trying to trace back the data in the Damned Lies thing. I went to the link to the first footnote here: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1005517/Technical_Briefing_19.pdf
And in there I find 224 deaths out of about 29k people who’ve had both shots, so 0.78%. Same math for the unvaccinated, 165 deaths out of 121k people, or 0.14%. And if you divide, the vaccinated have an IFR 5.7x the unvaccinated, is that his math when he says the following (I tweaked the emphasis in my quote from the original)? Footnote (1) is the link above.
" The real world data has shown that the death rate among the vaccinated, if infected with COVID, can be 3 to 5.7 times higher(1) than the death rate of the unvaccinated."
It’s confusing because those numbers add up, but then right below this is a chart showing vaccinated IFR of like 2%.
Yep, good question. I don’t know where that graph comes from. He mentions Israeli data that supports the 3X IFR figure (and the graph you point out seems to show vaccinated IFR at about 2% and unvaccinated at ~0.7%, which would work out to about 3X), but I don’t see a link to it, nor anything that supports a 2% IFR. The tables in the blog post, presumably taken from the Israeli data (or maybe UK?) certainly don’t support a 2% IFR from what I can tell.
I’m more worried about the 5.7x math. If I’m right about how he calculated it, using raw totals, it doesn’t control for age (which is the only breakout in the data). The unvaccinated skews very heavily towards age<50, while the vaccinated population is about evenly divided. The unvaccinated IFR is worse for both groups (just barely for <50), but Simpson’s paradox and all.
ETA: for age<50, the IFR is 0.026% for vaccinated vs 0.029% for unvaccinated. For 50+ it’s 1.64% for vaccinated vs 5.61% for unvaccinated.
I agree with his general point that we shouldn’t be saying vaccines reduce your risk by 90%+ once you contract COVID. But I’m not sure he’s pushing back correctly.
1 Like
I don’t think he’s trying to completely push back on the narrative, just to dig into the numbers a bit more and make sure people are more precise in what they’re saying about the numbers, especially so they can evaluate trends better. I think he would agree with you on the Simpsons paradox issue.
People saying things like “I’m vaccinated, therefore if I get Covid I’m protected from severe outcomes” are mistaken, given this data, which can lead to people taking more risks than they really intend to. (It’s also possible that cases/infections are being undercounted among the vaccinated if testing policies have changed & differ between the two groups, and maybe it really is the IFR where the benefit is. It’s just important not to double- or triple- or quadruple- count the benefit of reduced infections and think that applies downstream, too.)
3 Likes
Agree on the ‘double counting’ issue, you can’t just randomly pick an outcome and assume that the vaccinated folks always do 90% better.
I can’t decide how the over/under counting might work. I suppose some vaccinated people would be likely to assume they don’t have COVID and therefore less likely to get tested. But I’d also guess that vaccinated people might be more generally worried about COVID and more likely to get tested. I haven’t looked for or seen data on that.
Anywho, good article!
1 Like
Thanks!
So let’s promote health by giving people free Krispy Kreme! 
3 Likes
That probably is a good incentive for the obese.